CAR-T CELL THERAPY -
PATIENT GUIDE
CAR T-cell therapy is an advanced immunotherapy that engineers a patient’s T cells to recognize and destroy cancer cells in blood cancers.
analyticsAt a Glance
- check_circleRe-engineers patient T-cells to recognise and kill cancer cells
- check_circleFDA and NMPA approved for blood cancers including ALL and DLBCL
- check_circleChina leads globally in active CAR-T clinical trials and NMPA-approved products
- check_circleTargets CD19, BCMA, CD22, and emerging solid tumour antigens
What Is CAR-T Cell Therapy?
CAR-T cell therapy is an adoptive cell therapy that genetically engineers a patient's own T-cells to express a chimeric antigen receptor (CAR) — a synthetic protein that directs T-cells to recognize and destroy cancer cells. First conceptualized by Zelig Eshhar in the late 1980s and brought to clinical success by Carl June's group at Penn in 2010–2012, the first FDA approval (Kymriah for pediatric B-ALL) followed in August 2017.
“CAR-T therapy is a personalized, living medicine — a one-of-a-kind biological drug made from each patient's own cells, capable of persisting and acting long after a single infusion.”
Adoptive Cell Therapy
A class of cancer therapy using immune cells collected from the patient, manipulated outside the body, and reinfused to target cancer — CAR-T is the most clinically advanced form of this approach.
The CAR Construct
A chimeric antigen receptor combines an extracellular scFv antibody domain (which recognizes the cancer antigen), a hinge/transmembrane region, and intracellular signaling domains (CD3-zeta + co-stimulatory) — all in a single synthetic protein.
MHC-Independent Killing
Unlike natural T-cell receptors that require MHC presentation, the CAR's scFv domain recognizes unprocessed antigens directly on cancer cell membranes — bypassing a major immune evasion mechanism used by tumors.
Serial Killing & Persistence
After killing the first target cell, the CAR-T cell survives, proliferates, and kills successive targets — a phenomenon called serial killing. The cells can persist for years, acting as a living ongoing therapy.
Generations of CAR Design
Each generation adds signaling components that enhance persistence, proliferation, and tumour-microenvironment resistance. All currently approved products are second-generation CARs.
| Generation | Signaling Domains | Key Characteristic | Clinical Status |
|---|---|---|---|
| 1st Generation | CD3-zeta only | Kills target cells; poor proliferation and no persistence | Abandoned — not clinically viable |
| 2nd Generation | CD3-zeta + CD28 or 4-1BB | Standard of care. CD28 = faster response; 4-1BB = longer persistence | All 9 FDA-approved products; NMPA-approved products |
| 3rd Generation | CD3-zeta + CD28 + 4-1BB | Dual co-stimulation for enhanced signaling — higher activity in solid tumours | Active clinical trials; China leading solid tumour programs |
| 4th Generation (TRUCKs) | CD3-zeta + co-stim + cytokine gene cassette | Secretes IL-12 or other cytokines to remodel the immunosuppressive tumour microenvironment | Early-phase trials; active in China for solid tumours |
The Manufacturing Process: From Patient to Product
CAR-T manufacturing integrates cell collection, genetic engineering, expansion, quality control, and cold-chain logistics — all within a 3–6 week window.
- 1
Leukapheresis — Collecting T-Cells
The patient is connected to an apheresis machine that separates white blood cells from whole blood. The collected leukocytes are quality-assessed and shipped in temperature-controlled containers to the CAR-T manufacturing facility — in China or abroad.
- 2
T-Cell Activation & Viral Transduction
T-cells are activated using anti-CD3/CD28 antibodies, then transduced with a viral vector (typically lentiviral) carrying the CAR gene. The CAR integrates permanently into the T-cell DNA and is passed to all daughter cells.
- 3
Expansion in Bioreactors
CAR-T cells are expanded over 7–14 days using IL-2 and growth factors to reach the target dose of 50 million to several hundred million cells per infusion.
- 4
Quality Control & Release Testing
Sterility, identity (confirmed CAR+ T-cells), viability, potency, and mycoplasma testing must all pass specifications before release. A significant percentage of autologous manufacturing runs fail QC — most often in heavily pre-treated patients with poor T-cell health.
- 5
Cold-Chain Shipping to Treatment Centre
The cryopreserved product is shipped back to the treating hospital under strict temperature-controlled conditions. Chinese manufacturers including Fosun Kite and Legend Biotech operate end-to-end cold-chain logistics for international patients.
- 6
Lymphodepletion Chemotherapy
Fludarabine and cyclophosphamide are given for 3 days (5–3 days before infusion) to deplete the patient's immune cells, eliminate suppressor cells, and create a homeostatic cytokine environment that drives CAR-T expansion in vivo.
- 7
CAR-T Infusion & Post-Infusion Monitoring
Infusion is similar to a blood transfusion — IV, 30–60 minutes. CRS and ICANS monitoring begins immediately: daily temperature checks, blood tests every 2–3 days, ferritin/CRP/LDH/cytokine panels as early CRS warning signals. Inpatient monitoring: 2–4 weeks.
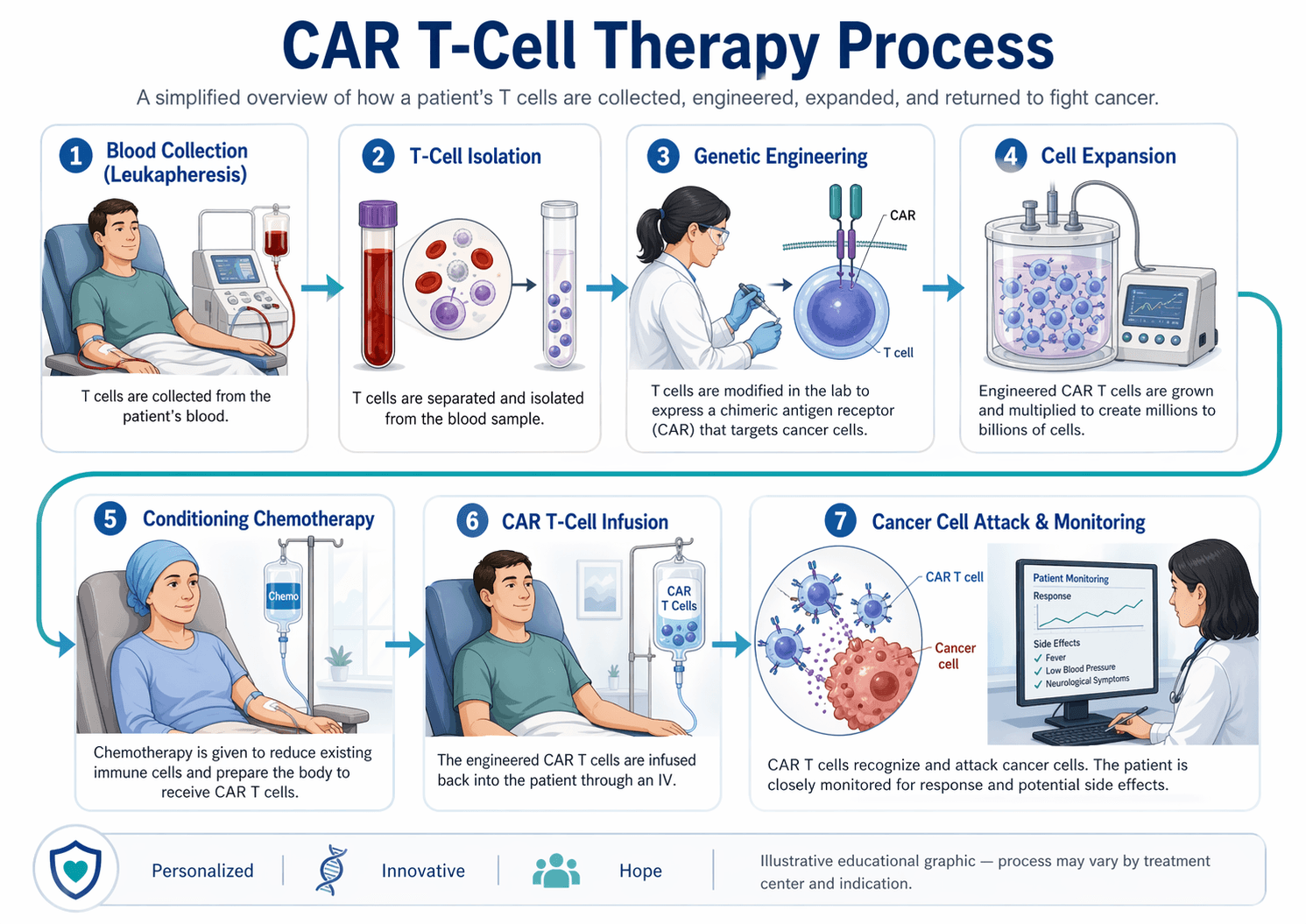
CAR T-Cell Therapy Process
CAR T-cell therapy is a personalized cancer treatment. First, doctors collect the patient’s T cells, which are important immune cells, through a blood collection process. These cells are then modified in a specialized laboratory so they can recognize a specific marker on cancer cells. After modification, the CAR T cells are multiplied in large numbers and carefully tested for quality. The patient may receive short chemotherapy to prepare the body. Finally, the CAR T cells are infused back into the patient, where they search for and attack cancer cells under close medical monitoring.
“CAR T-cell therapy collects a patient’s immune cells, genetically trains them to recognize cancer, expands them in a lab, and then infuses them back to attack cancer cells under specialist supervision.”
FDA & NMPA Approved CAR-T Products
As of 2025, nine CAR-T products are FDA-approved. Not all are available in all countries — patients outside the US and Europe should verify local availability or explore China and clinical trial pathways.
| Product (Brand) | Target | Approved Indication(s) | Key ORR |
|---|---|---|---|
| Tisagenlecleucel (Kymriah) | CD19 | Pediatric/YA B-ALL; r/r DLBCL; FL | 81% CR in B-ALL (ELIANA) |
| Axicabtagene ciloleucel (Yescarta) | CD19 | r/r DLBCL; FL; MCL | 83% ORR in DLBCL (ZUMA-1) |
| Lisocabtagene maraleucel (Breyanzi) | CD19 | r/r DLBCL; FL; MCL; CLL/SLL | 73% ORR in DLBCL (TRANSCEND) |
| Brexucabtagene autoleucel (Tecartus) | CD19 | Adult r/r B-ALL; MCL | 71% ORR in MCL (ZUMA-2) |
| Ciltacabtagene autoleucel (Carvykti) | BCMA | r/r Multiple Myeloma (≥1 prior line) | 97.9% ORR (CARTITUDE-1) |
| Idecabtagene vicleucel (Abecma) | BCMA | r/r Multiple Myeloma (≥4 prior lines) | 73% ORR (KarMMa) |
| Relma-cel (JWCAR029) — NMPA | CD19 | r/r B-ALL; DLBCL (China) | Published Phase II data |
| Equecabtagene autoleucel — NMPA | BCMA | r/r Multiple Myeloma (China) | Approved 2023 |
| Inaticabtagene autoleucel — NMPA | BCMA | r/r Multiple Myeloma (China) | Approved 2023 |
Clinical Efficacy Data by Indication
Key response data from pivotal trials underpinning FDA approvals. All in heavily pre-treated, relapsed/refractory patients.
B-ALL — ELIANA Trial (Kymriah)
Pediatric and young adult r/r B-ALL. 60% of responders MRD-negative.
DLBCL — ZUMA-1 Trial (Yescarta)
r/r large B-cell lymphoma after ≥2 prior therapies.
Multiple Myeloma — CARTITUDE-1 (Carvykti)
r/r MM after ≥4 prior lines including PI, IMiD, anti-CD38.
Multiple Myeloma — KarMMa (Abecma)
r/r MM after ≥4 prior lines.
CAR-T Cell Therapy: Key Numbers
- 9FDA-Approved CAR-T Products (2025)Covering B-ALL, DLBCL, FL, MCL, and multiple myeloma.
- 97.9%Highest ORR — Carvykti in r/r MyelomaCARTITUDE-1 trial; best published CAR-T response rate to date.
- 3–6 weeksAutologous Manufacturing TimeChinese manufacturers (Fosun Kite, Legend Biotech) operate at the faster end of this range.
- 30–50%Cost Saving in China vs USAFor NMPA-approved equivalent CAR-T products at leading Chinese haematology centres.
- 21.8Median Duration of ResponseAmong responders in CARTITUDE-1, the median duration of response was 21.8 months, which pairs well with the headline ORR and adds an important durability number.
- 1 monthMedian Time to First ResponseResponses appeared quickly, with a median time to first response of 1 month in the FDA label, which is a useful practical benchmark for patient-facing content.
Key Toxicities: CRS vs ICANS
CAR-T has a unique side-effect profile unlike chemotherapy or checkpoint immunotherapy. Both major toxicities are graded, monitored, and — in experienced centres — managed predictably.
Cytokine Release Syndrome (CRS)
- Occurs in 50–90% of patientsRanging from mild fever to life-threatening vasopressor-dependent hypotension.
- Caused by massive cytokine releaseCAR-T activation triggers IL-6, IFN-γ, and TNF release from bystander immune cells.
- Grades 3–4: immediate interventionTocilizumab (anti-IL-6R) is first-line; corticosteroids for refractory cases.
- Fully reversible in most casesWith experienced management; Grade 3–4 CRS is rare with 2nd-gen CD19 products.
Neurotoxicity (ICANS)
- Encephalopathy, aphasia, tremorsRanges from mild confusion and word-finding difficulties to seizures and brain oedema.
- Graded by ASTCT ICANS scaleCognitive status, language, attention, writing, and level of consciousness assessed.
- Grade 1–2: close monitoringSupportive care; usually resolves spontaneously.
- Grade 3–4: corticosteroids urgentDexamethasone or methylprednisolone; ICU care for severe cases. Rare with current products.
CAR-T for Solid Tumours: The Next Frontier
Extending CAR-T to solid tumours is the most important unsolved challenge in the field. Three barriers — antigen heterogeneity, poor tumour infiltration, and an immunosuppressive microenvironment — require next-generation solutions. China leads global clinical trial activity for solid tumour CAR-T.
GD2 — Neuroblastoma & Osteosarcoma
Highly expressed on neuroblastoma, osteosarcoma, and melanoma. Anti-GD2 CAR-T has shown early responses in pediatric neuroblastoma (Great Ormond Street, US centres). Chinese groups have active GD2 programmes.
HER2 — Breast, Gastric, Glioblastoma
Overexpressed in HER2+ breast, gastric, and other cancers. Must be carefully dosed to avoid pulmonary on-target toxicity. Promising early data in HER2+ glioblastoma, where the brain environment provides partial immune privilege.
Mesothelin — Mesothelioma, Ovarian, Pancreatic
Expressed on mesothelioma, ovarian, lung adenocarcinoma, and pancreatic cancer. Phase I trials show safety and modest activity. Chinese centres have active mesothelin CAR-T programmes.
EGFR / EGFRvIII — NSCLC, Glioblastoma
EGFRvIII is a tumour-specific mutant expressed on glioblastoma — not on normal tissue. Wild-type EGFR programmes in NSCLC and colorectal cancer have been pioneered by Chinese groups at the PLA General Hospital. Early published data are promising.
China's CAR-T Programme: World's Largest
Between 2016 and 2024, China registered more CAR-T clinical trials than any other country. Multiple domestic products are NMPA-approved, with Chinese companies leading proprietary manufacturing innovations.
“"China's CAR-T programme is reshaping global access to cell therapy—offering more approved products, broader clinical trials, and significantly lower costs than any other country. For patients with relapsed blood cancers who have run out of standard options, China represents one of the most important treatment frontiers in the world today."”
China has the largest CAR-T cellular treatment program in the world, with more CAR-T treatments approved compared to other countries, along with a large number of clinical trials covering more types of cancer than can be found within the reach of the US and European patients. The US only has six FDA-approved CAR-T treatments that are primarily for certain types of blood cancers. China, on the other hand, has several CAR-T treatments approved, including those for B-cell cancers and BCMA-targeted treatments for multiple
The reasons why the Chinese program stands out compared to other countries in relation to foreign patients include the number of participants, affordability, and diversity of treatment choices. The cost of CAR-T treatment in China is only a small portion of what it could be in the US, where an individual procedure can cost more than $400,000 without even including hospital fees. Some Chinese institutes like those attached to the university hospitals in Shanghai, Beijing, and Guangzhou are using advanced CAR-T treatments, two targets, and new antigens.
For patients with relapsed or refractory blood cancers who have exhausted standard options, China's CAR-T programme represents one of the most active global hubs for both approved treatment and clinical trial access, a pathway CancerFax helps eligible patients navigate.
Fosun Kite (Yescarta equivalent)
Fosun Kite's axicabtagene ciloleucel (axi-cel) is NMPA-approved for r/r DLBCL and FL — the Chinese equivalent of Yescarta, manufactured domestically with established cold-chain logistics for international patients.
Legend Biotech / Carvykti (BCMA)
Legend Biotech (Nanjing) developed the LCAR-B38M nanobody-based BCMA CAR-T (now Carvykti globally). This Chinese-origin product achieved the highest ORR ever published for a CAR-T therapy: 97.9% in r/r myeloma.
Gracell's FasT CAR Platform
Gracell Biotechnologies' proprietary FasT CAR platform reduces standard manufacturing time from 14–21 days to 22–36 hours — potentially transforming access for patients who cannot wait weeks for product manufacturing.
CD7 CAR-T for T-Cell Malignancies
Chinese groups (Wuhan Union Hospital) have pioneered CD7-targeted CAR-T for T-cell ALL and T-cell lymphoma — a previously untreatable indication with dramatic published Phase I/II results.
Cost Comparison: China vs USA vs Europe
For most international patients from South Asia, the Middle East, and Southeast Asia, China is the most practical access pathway — combining NMPA-approved products, domestic manufacturing, and substantially lower cost.
| Cost Component | USA | Europe (Germany) | China |
|---|---|---|---|
| CD19 CAR-T Product (DLBCL) | $373,000–$475,000 | €320,000–€380,000 | ¥1.2M–¥1.5M (~$165K–$205K) |
| BCMA CAR-T Product (Myeloma) | $465,000–$500,000 | €400,000–€450,000 | ¥1.5M–¥2M (~$205K–$275K) |
| Hospital & Monitoring (30 days) | $80,000–$150,000 | €50,000–€80,000 | ¥200K–¥400K (~$28K–$55K) |
| Lymphodepletion Chemo | $10,000–$20,000 | €8,000–€15,000 | ¥30K–¥60K (~$4K–$8K) |
| Estimated All-In Total | $500K–$700K | €400K–€550K | $200K–$350K (USD equiv.) |
| Insurance Coverage | Medicare/commercial (partial) | Public health (partial) | Self-pay; CancerFax assistance |
Know CAR T-Cell Therapy in Detail
Explore in-depth guides on every aspect of CAR-T cell therapy.
- What is CAR-T Cell Therapy?
- How CAR-T Therapy Works
- CAR-T vs Bone Marrow Transplant
- CAR-T vs TIL Therapy
- Cancers Treated with CAR-T Therapy
- CAR-T Therapy for Leukemia
- CAR-T Therapy for Lymphoma
- CAR-T Therapy for Multiple Myeloma
- CAR-T Therapy for Solid Tumors
- Eligibility for CAR-T Therapy
- Tests Required Before CAR-T Therapy
- CAR-T Treatment Process
- Hospital Stay for CAR-T Therapy
- Side Effects of CAR-T Therapy
- Cytokine Release Syndrome Explained
- Success Rates of CAR-T Therapy
- Cost of CAR-T Therapy Worldwide
- CAR-T Clinical Trials
- Future of CAR-T Therapy
- Questions Patients Should Ask
Frequently Asked Questions
The most common questions from patients and families exploring CAR-T cell therapy.
Basics
Eligibility & Access
Side Effects & Safety
Cost & Logistics
How CancerFax Helps
CancerFax is a specialist cancer access and patient-navigation platform. We help patients and families understand their options, organise medical records, coordinate hospital communication, and support cross-border treatment planning where appropriate.
We help collect and organise reports, scans, pathology, biomarker results, and treatment history for structured case review.
We communicate with hospitals or trial teams to assess whether a case may be suitable for further screening.
We support appointment coordination, document submission, translation, and direct communication with international departments.
For international patients, we help with practical coordination — travel planning, hospital admission guidance, and local support.
If this option is not suitable, we help explore other relevant treatments, clinical trials, or advanced care pathways.
From inquiry through to follow-up, our coordinators provide a single point of contact for the family.
CancerFax does not guarantee treatment access, eligibility, or clinical outcome. Our role is to help patients access accurate information, structured review, and appropriate specialist pathways.
Is CAR-T Cell Therapy an Option for Your Case?
Upload your haematology reports and our oncology navigation team will assess eligibility for FDA- and NMPA-approved CAR-T products and identify open clinical trials within 48 hours.
This content is for informational purposes only and does not constitute medical advice. Always consult a qualified haematologist or oncologist before making treatment decisions.