Non-Hodgkin Lymphoma (NHL)
There are many different kinds of lymphomas, including more than 60 lymphoid neoplasms, such as follicular lymphoma that can be treated for many years using mild treatments, diffuse large B-cell lymphoma, which needs immediate immunochemotherapy, and other forms of relapsing lymphomas that have been revolutionized by CAR-T cells and bispecific antibodies.
- Subtype and molecular profile drive every treatment decision
- CAR-T cell therapy access coordinated globally
- Bispecific antibody and BTK inhibitor access navigated
- Expert lymphoma second opinions arranged
- Most Common Aggressive Subtype
- DLBCL — ~25–30% of all NHL worldwide
- Lineage Split
- ~85% B-cell NHL · ~15% T-cell and NK-cell NHL
- Key Tests
- Biopsy · IHC · FISH · NGS · PET-CT · Cell of Origin (COO)
- Advanced Therapies
- CAR-T · Bispecific Abs · BTK inhibitors · EZH2 inhibitors
- Critical Factor
- Histologic subtype and molecular risk classification
What is Non-Hodgkin Lymphoma (NHL)
Types and Subtypes of Non-Hodgkin Lymphoma
According to the WHO Classification of NHL (2022), there are more than 60 types of NHL, which may occur depending upon the type of cells from where it originated, its morphology, and the immunological as well as genetic makeup. As far as the clinical classification of NHL is concerned, it can be classified into B cell lymphomas (most commonly occurring) and T-/NK-cell lymphomas. In case of B-cell lymphomas, it can again be divided into aggressive and indolent NHLs.
Symptoms and Signs
NHL symptoms differ depending on various factors such as the subtype of NHL, the site where it occurs, its prevalence, and the rate of progression. For example, with indolent NHL, the patient may show less evident symptoms over a span of months or years. There are some cases in which the disease occurs randomly when conducting an examination for another condition. With aggressive NHL, the symptoms manifest themselves quickly within days or weeks.
Extranodal NHL occurring in the gastrointestinal tract, brain, skin, bone marrow, and mediastinum causes symptoms that are not suggestive of NHL.
Examples of "B" symptoms include fever, sweating at night, and weight loss in excess of 10% of the body mass.
Causes and Risk Factors
The etiology of NHL differs from subtype to subtype, with several etiologies still unestablished for almost all subtypes. The etiology of solid tumors may vary from exposure to carcinogens to something else. But in the case of NHL, the development is influenced by more than one factor, such as genetics, immune response, infections, and sometimes antigenic response.
Certain infections have been shown to be a cause for certain NHL subtypes; for example, EBV infection causes Burkitt lymphoma and NK/T cell lymphoma, H. pylori infection causes gastric MALT lymphoma, HTLV-1 causes adult T-cell leukemia/lymphoma, and HHV8 causes primary effusion lymphoma. These are significant from a treatment point of view because the removal of H. pylori infection alone can cure early-stage gastric MALT lymphoma.
Diagnosis and Investigations
NHL is detected through a biopsy; nevertheless, it is pertinent to understand that, in this scenario, a fine needle aspiration is not sufficient since there is a requirement for immunophenotyping, architecture evaluation, and molecular assessment so that NHL can be classified into different categories. An excisional lymph node biopsy/core needle biopsy (proper gauge size) is taken in this case. After that, the pathological analysis and the subsequent molecular and staging analysis should take place, with the PET-CT scan being a mandatory procedure in most cases of NHL.
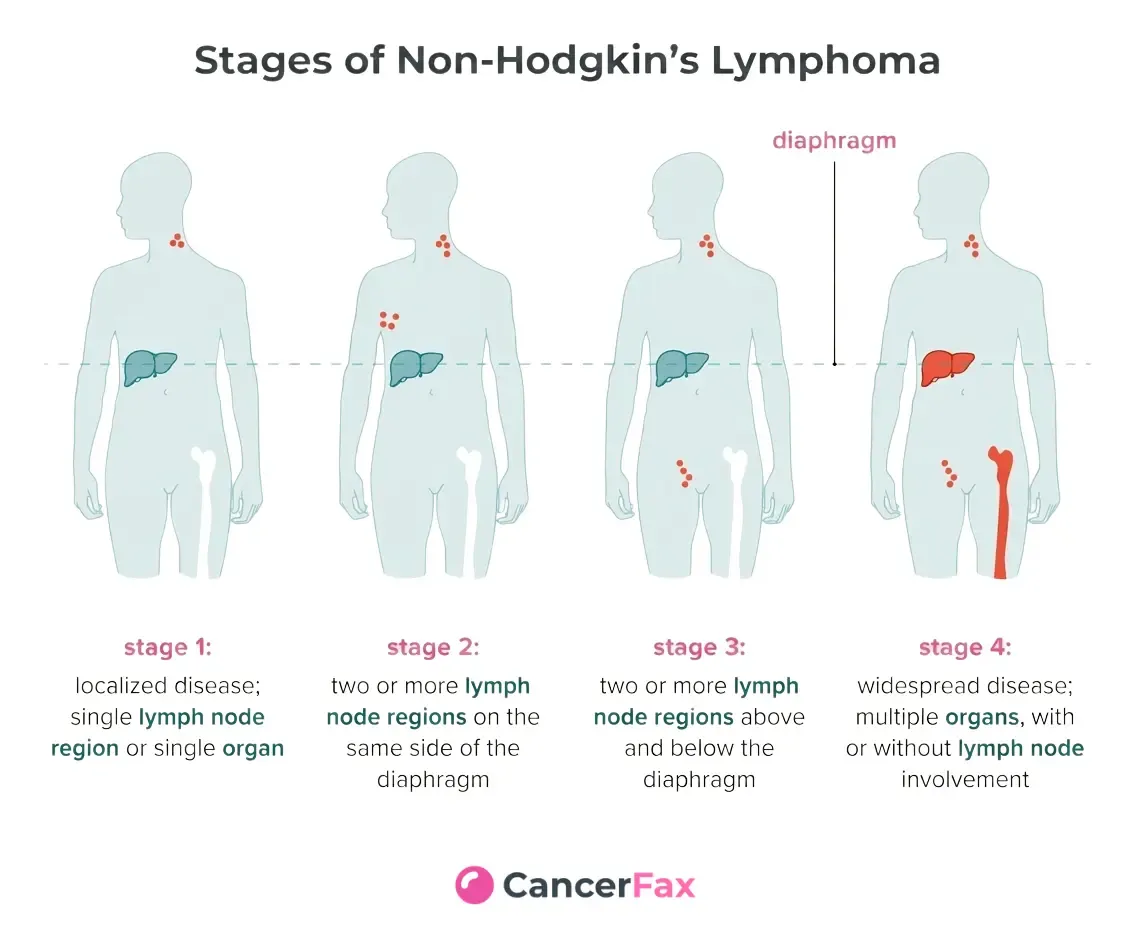
Staging — Ann Arbor / Lugano Classification
NHL staging is performed using the Ann Arbor Classification, which was updated to the Lugano Classification in 2014, with the stages depending on how much the disease has spread in terms of anatomy, starting with stage I (disease localized in only one area of a lymph node) and ending with stage IV (the disease is widely spread in extranodal sites).
FDG-positive lymphomas are staged using the PET-CT imaging test, while non-FDG-positive lymphomas are staged using CT. Any patient with B symptoms, such as fever, profuse sweating at night, and more than 10% weight loss, receives the designation B in addition to their diagnosis.
Standard Treatment
NHL treatment is dependent on the type of NHL and not the generic NHL treatment protocol. Treatment for NHL could range from a ‘Watch and Wait' treatment protocol for asymptomatic indolent NHL with low tumor burden to chemotherapy along with Rituximab (anti-CD20 antibody) for majority B-cell NHL cases, while aggressive chemotherapy protocols may be used for aggressive NHLs and double-hit lymphomas.
While ASCT still stands out as a standard treatment modality for consolidation treatment in patients with aggressive NHL after salvage treatment, recent novel therapies, including Chimeric Antigen Receptor-T (CAR-T) cells for relapse DLBCL patients, have been developed.
Advanced & Emerging Therapies
During the last decade, the NHL has seen a massive rise in the number of new agents approved; this has led to a great deal of innovation. The CAR T-cell therapy is now the main mode of treatment for patients with DLBCL; there are powerful off-the-shelf CAR T cells in the form of bispecific antibodies. The BTK inhibitors have ushered in a revolution in the treatment of MCL, MZL, and WM; EZH2 inhibitors are the first targeted molecules in follicular lymphoma, while Polatuzumab vedotin is the main agent in the ADC of NHL.
Cellular Therapy — CAR-T
Axicabtagene Ciloleucel (Axi-cel) / Lisocabtagene Maraleucel (Liso-cel) / Tisagenlecleucel
CD19-targeted autologous CAR-T cell therapies approved for relapsed/refractory DLBCL (all three), follicular lymphoma (axi-cel, Grade 1–2; liso-cel), and mantle cell lymphoma (brexucabtagene autoleucel — a related product). Axi-cel and liso-cel are also approved in the second-line DLBCL setting, having demonstrated superiority over salvage chemotherapy followed by ASCT in primary refractory or early relapsed disease. Requires specialized center with CAR-T program and management of cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS).
Bispecific Antibody (CD20xCD3)
Epcoritamab / Glofitamab
Off-the-shelf bispecific CD20xCD3 T-cell engager antibodies approved for relapsed/refractory DLBCL and other large B-cell lymphomas after two or more prior lines. Epcoritamab (subcutaneous) and glofitamab (intravenous, fixed duration 12 cycles) both produce meaningful response rates in heavily pretreated patients. Key advantage over CAR-T: no manufacturing wait time. Cytokine release syndrome (CRS) is the primary toxicity, managed with step-up dosing and hospitalization for early cycles.
Bispecific Antibody (CD20xCD3) — Indolent NHL
Mosunetuzumab
A bispecific CD20xCD3 antibody approved for relapsed/refractory follicular lymphoma after two or more prior therapies. Fixed-duration treatment (8 cycles) produces complete response rates significantly higher than historical benchmarks in this population. An important advance for patients with relapsed FL who do not have CAR-T access or who prefer a fixed-duration approach.
Targeted Therapy (BTK Inhibitor)
Zanubrutinib / Ibrutinib / Acalabrutinib
Bruton tyrosine kinase (BTK) inhibitors are approved across multiple NHL subtypes. Zanubrutinib (second-generation, more selective) and ibrutinib are both approved for mantle cell lymphoma, marginal zone lymphoma, and Waldenström macroglobulinemia. Zanubrutinib has demonstrated superiority over ibrutinib in WM and CLL/SLL with improved tolerability. BTK inhibitors are now incorporated into first-line MCL regimens and represent standard therapy for relapsed/refractory MZL and WM.
ADC (Antibody-Drug Conjugate)
Polatuzumab Vedotin (Pola-R-CHP)
An anti-CD79b ADC delivering MMAE directly to B-cells. The pola-R-CHP regimen (polatuzumab vedotin + rituximab + cyclophosphamide, doxorubicin, prednisone, replacing vincristine) is approved as first-line treatment for DLBCL, demonstrating improved progression-free survival over R-CHOP in the POLARIX trial. Also used in relapsed/refractory settings in combination with bendamustine + rituximab.
Targeted Therapy (EZH2 Inhibitor)
Tazemetostat
A selective EZH2 methyltransferase inhibitor approved for relapsed/refractory follicular lymphoma — specifically for EZH2-mutant FL (with higher response rates) and EZH2 wild-type FL after two or more prior therapies. EZH2 mutations occur in approximately 20–25% of follicular lymphoma (enriched in GCB subtype). Tazemetostat is the first molecularly targeted agent with approved biomarker-selected use in follicular lymphoma. Well tolerated orally.
Targeted Therapy (BCL2 Inhibitor)
Venetoclax (in MCL and indolent B-cell NHL)
A BCL2 inhibitor that induces apoptosis in BCL2-overexpressing lymphoma cells. Approved for CLL/SLL; used off-label or in trials for mantle cell lymphoma (venetoclax + ibrutinib combination has shown high response rates) and other indolent B-cell lymphomas. Tumor lysis syndrome prophylaxis is required with ramp-up dosing.
ADC (Antibody-Drug Conjugate) — CD30-Targeted
Brentuximab Vedotin (in ALCL and other CD30+ NHL)
An anti-CD30 ADC delivering MMAE to CD30-expressing lymphoma cells. Brentuximab vedotin combined with CHP (A+CHP) is the approved first-line regimen for systemic ALCL (ALK+ and ALK-) and other CD30-positive T-cell lymphomas. Also used in relapsed/refractory CD30-positive DLBCL and as a bridge to transplant or CAR-T in relapsed settings.
Cellular Therapy (Allogeneic CAR-T — Emerging)
Allogeneic and Next-Generation CAR-T Programs
Multiple clinical programs are developing allogeneic ('off-the-shelf') CAR-T cells from healthy donor T-cells, which would eliminate the manufacturing wait time of autologous CAR-T. China has been a leader in CAR-T development and is running multiple trials including FasT CAR-T programs with next-day manufacturing, dual-targeting CAR-T (CD19+CD22), and armored CAR-T constructs — accessible through specialist centers for patients who have exhausted standard options.
Biomarkers & Precision Medicine
The NHL testing may include biomarker classes as follows: firstly, diagnostic biomarkers that help identify a subtype (CD20, cyclin D1, ALK); secondly, prognostic biomarkers used to predict specific prognosis within the subtype (IPI, double hit, Ki-67); and, thirdly, predictive biomarkers that will be used to choose a certain drug (EZH2 mutation for tazemetostat, MYD88 L265P mutation for a BTK inhibitor in WM/ABC DLBCL, and CD19 for CAR-T). It is ideal that all tests be carried out before treatment begins (IHC; FISH, where applicable; and NGS).
When to Seek a Second Opinion
Heterogeneous diseases have been associated with NHL, and as such, it becomes crucial to classify the various types of diseases to be able to treat them effectively. In light of the difficulties associated with diagnosis and the fact that the treatment regimen varies and that some patients lack access to novel treatments like CAR-T, bispecific medications, and BTK inhibitors, different situations require an expert assessment at a lymphoma center.
Clinical Trials & Research
Prognosis & Outcome Factors
It has been observed that the prognosis for NHL is highly dependent on the NHL subtype, as there exist more than 60 NHL subtypes, with a varying prognosis for each subtype. It has been widely acknowledged that indolent NHL cannot be cured by chemotherapy; however, the advent of new therapies has led to increased periods of remissions and better survival with improved quality of life. Conversely, aggressive NHLs, including DLBCL, can easily be cured with primary therapies involving both chemotherapies and immunotherapies.
These therapies have brought about remissions even among patients with NHL, despite them being resistant to other forms of treatment. However, it can still be said that the prognosis for T-cell NHL remains dire.
Supportive Care & Living With Non-Hodgkin Lymphoma
The management of NHL, which may require some months with aggressive immunochemotherapy, new agents, and possibly even CAR-T cell therapy, should involve a holistic approach to supporting care during the entire process of management, from the beginning through the completion of treatment. These are among the possible complications that might arise in relation to NHL treatments:
• Infections caused by the decline of B-cells because of rituximab
• Cytokine release syndrome, which may be triggered by CAR-T and bispecifics
• Peripheral neuropathy due to vincristine or brentuximab vedotin
• Heart complications caused by anthracyclines
• Immunosuppression
How CancerFax Helps You Explore Treatment Options
CancerFax supports NHL patients and families by reviewing biopsy reports, IHC panels, FISH results, NGS profiling, PET-CT staging, and treatment history to establish the exact lymphoma subtype and molecular risk profile — and to identify which treatment options, from R-CHOP to CAR-T cell therapy, bispecific antibodies, BTK inhibitors, EZH2-targeted therapy, and clinical trials at specialist centers in China and globally, may be relevant for your specific diagnosis.
Get a free case reviewFrequently Asked Questions
Non-Hodgkin lymphoma (NHL) is a broad term covering more than 60 distinct malignancies that arise from lymphocytes — the white blood cells of the immune system. B-cell lymphomas account for approximately 85% of NHL; T-cell and NK-cell lymphomas make up the remaining 15%. NHL is characterized by the clonal proliferation of lymphocytes that have undergone malignant transformation at various stages of their development.
Hodgkin lymphoma (HL) is a distinct entity defined by the presence of Reed-Sternberg cells — large abnormal B-cells with a characteristic 'owl-eye' appearance on biopsy. HL is generally more predictably curable with standard chemotherapy (ABVD or BEACOPP) and is highly sensitive to checkpoint immunotherapy. NHL, by contrast, is biologically diverse — ranging from indolent diseases managed for years to aggressive lymphomas requiring urgent intensive treatment. The two categories have different epidemiology, clinical behavior, and treatment approaches.
NHL diagnosis requires a tissue biopsy — fine needle aspiration (FNA) alone is not sufficient. An excisional lymph node biopsy (removing an intact lymph node) or a core needle biopsy with multiple passes provides the tissue needed for comprehensive evaluation. The biopsy specimen undergoes: morphologic assessment by a hematopathologist; immunohistochemistry (IHC) with a comprehensive antibody panel; FISH for key chromosomal rearrangements (MYC, BCL2, BCL6, CCND1, ALK); and, in many centers, an NGS panel for mutational profiling.
Beyond the biopsy, the workup includes PET-CT staging, bone marrow biopsy, blood tests (LDH, beta-2 microglobulin, full blood count, liver and kidney function), EBV serology, HIV testing, and hepatitis B/C serology — with lumbar puncture for CNS assessment in high-risk aggressive NHL. This comprehensive approach takes time but is essential — initiating treatment before the subtype is fully characterized risks using the wrong protocol.
Aggressive NHL — including DLBCL, mantle cell lymphoma, and Burkitt lymphoma — grows rapidly and, if untreated, can be life-threatening within weeks to months. It requires urgent initiation of intensive treatment. The good news is that many aggressive NHL subtypes are potentially curable: approximately 60% of DLBCL patients are cured with first-line R-CHOP or pola-R-CHP.
Indolent NHL — including follicular lymphoma, marginal zone lymphoma, and lymphoplasmacytic lymphoma — grows slowly, often over years. While generally not curable with standard therapy, it can be managed effectively for many years. A critical principle in indolent NHL is that immediate treatment is not always necessary — for asymptomatic patients with low tumor burden, watchful waiting ('watch and wait') is appropriate and delays treatment toxicity without harming outcomes. The treatment approach in indolent NHL is calibrated to the patient's symptoms and disease burden, not the stage alone.
Double-hit lymphoma — formally called High-Grade B-Cell Lymphoma with MYC and BCL2 rearrangements (HGBL) — is a distinct and aggressive category of large B-cell lymphoma defined by concurrent chromosomal rearrangements of both the MYC gene and the BCL2 gene. These concurrent rearrangements simultaneously activate a powerful growth driver (MYC) and block apoptosis (BCL2), producing a uniquely aggressive tumor biology.
Double-hit lymphoma is clinically important because it does not respond as well to standard R-CHOP as conventional DLBCL, and patients treated with R-CHOP alone have significantly worse outcomes. Intensified regimens — most commonly DA-R-EPOCH — are used instead. FISH testing for MYC and BCL2 (and BCL6 for 'triple-hit') is mandatory in all newly diagnosed DLBCL. If this testing was not done at your diagnosis, or results are missing, this should be urgently addressed before treatment planning is finalized.
CAR-T (chimeric antigen receptor T-cell) therapy is a personalized cellular immunotherapy in which the patient's own T-cells are collected, genetically engineered in a laboratory to express a receptor that recognizes the CD19 protein on lymphoma cells, and then infused back into the patient after lymphodepleting chemotherapy. The engineered T-cells multiply and attack CD19-expressing lymphoma cells. Three CAR-T products are approved for NHL: axicabtagene ciloleucel (axi-cel), tisagenlecleucel (tisa-cel), and lisocabtagene maraleucel (liso-cel) — each with somewhat different risk profiles and approved indications.
CAR-T is currently approved for relapsed or refractory DLBCL and follicular lymphoma after two or more prior lines of therapy, and — based on recent trial data — for second-line DLBCL that is primary refractory or early relapsed (within 12 months of first-line). Eligibility requires CD19-positive disease, adequate organ function, and absence of active CNS lymphoma. Manufacturing requires approximately 3–4 weeks; patients may receive bridging therapy during this period. CAR-T requires specialist center infrastructure and is not universally available — CancerFax can assist in identifying centers and supporting international coordination.
Bispecific CD20xCD3 antibodies — including epcoritamab and glofitamab (for DLBCL) and mosunetuzumab (for follicular lymphoma) — simultaneously bind CD20 on lymphoma cells and CD3 on T-cells, physically bringing a T-cell into close proximity with the lymphoma cell and activating the T-cell to kill it. Unlike CAR-T, bispecific antibodies are 'off-the-shelf' ready-made drugs that do not require personalized manufacturing — they can be started within days rather than weeks.
Bispecific antibodies produce meaningful response rates in relapsed/refractory DLBCL and FL. Their primary toxicity is cytokine release syndrome (CRS) — managed with step-up dosing and hospitalization for early cycles. They represent an important alternative for patients who cannot wait for CAR-T manufacturing, who have had prior CAR-T, or who are treated at centers without CAR-T programs. Ongoing trials are evaluating bispecific antibodies in earlier lines and in combination with standard chemoimmunotherapy.
Not necessarily. For patients with asymptomatic, low-tumor-burden follicular lymphoma — defined by criteria such as no B symptoms, no rapidly enlarging nodes, no organ compromise, no significant bone marrow failure, and no large tumor masses — active surveillance ('watch and wait') is an appropriate and evidence-based initial strategy. Multiple clinical trials have confirmed that immediate treatment of asymptomatic low-tumor-burden FL does not improve survival compared to deferred treatment when symptoms or disease progression develops.
Watch and wait means regular monitoring (typically every 3 months initially, then less frequently if stable) with clinical assessment and periodic imaging. Treatment is initiated when defined criteria are met: symptoms develop, disease bulk increases significantly, organ function is threatened, or hematologic parameters worsen. When treatment is initiated, rituximab-based chemoimmunotherapy (typically bendamustine + rituximab) followed by rituximab maintenance is the current standard for advanced-stage symptomatic FL. For relapsed EZH2-mutant FL, tazemetostat provides a targeted molecular option.
Yes — NHL is one of the most active areas of hematologic oncology research globally, and China has particular importance in this space, especially for cellular therapies. China has been a global pioneer in CAR-T cell therapy development and has multiple active trials that are not yet available in other countries: FasT CAR-T programs with very short manufacturing timelines (as little as 24 hours), dual-targeting CAR-T products (CD19+CD22 or CD19+CD20) designed to prevent antigen escape, and 'armored' CAR-T constructs with improved T-cell persistence and effector function. Multiple phase II and III trials are running at centers such as Beijing's CAMS, Peking University Cancer Hospital, and Ruijin Hospital in Shanghai.
Beyond China, active international trial areas include first-line bispecific antibody combinations, MRD-guided therapy de-escalation in FL, T-cell lymphoma-specific programs (IDH2 inhibitors in AITL, ALK inhibitors in ALCL), and allogeneic CAR-T. CancerFax can assist in reviewing your NHL subtype and treatment history against open trial criteria and facilitating contact with enrolling centers, including in China.
Yes. CancerFax supports NHL patients and families through the complete treatment navigation process. We start with a detailed review of your biopsy report, IHC panel, FISH results, NGS profiling, PET-CT staging, and treatment history to establish your exact lymphoma subtype, molecular risk classification, and disease status — because in NHL, these details determine everything about which treatment is appropriate.
Based on this review, we identify which standard and advanced treatment options apply — from R-CHOP or pola-R-CHP for newly diagnosed DLBCL, to rituximab maintenance and watch-and-wait for indolent FL, to BTK inhibitors for MCL or WM, tazemetostat for EZH2-mutant FL, and CAR-T cell therapy or bispecific antibodies for relapsed disease. We coordinate second opinion consultations with specialist lymphoma hematologists and facilitate international treatment navigation for patients seeking access to CAR-T programs, clinical trials, or specialist centers in India, China, or globally. Send your medical reports to get started.